Students with Reactive Attachment Disorder often need a unique plan to help find them success at school. This post aims to help bring understanding and ideas to support your students with Reactive Attachment Disorder.
MAYO CLINIC
Overview
Reactive attachment disorder is a rare but serious condition in which an infant or young child doesn’t establish healthy attachments with parents or caregivers. Reactive attachment disorder may develop if the child’s basic needs for comfort, affection and nurturing aren’t met and loving, caring, stable attachments with others are not established.
With treatment, children with reactive attachment disorder may develop more stable and healthy relationships with caregivers and others. Treatments for reactive attachment disorder include psychological counseling, parent or caregiver counseling and education, learning positive child and caregiver interactions, and creating a stable, nurturing environment.
Symptoms
Reactive attachment disorder can start in infancy. There’s little research on signs and symptoms of reactive attachment disorder beyond early childhood, and it remains uncertain whether it occurs in children older than 5 years.
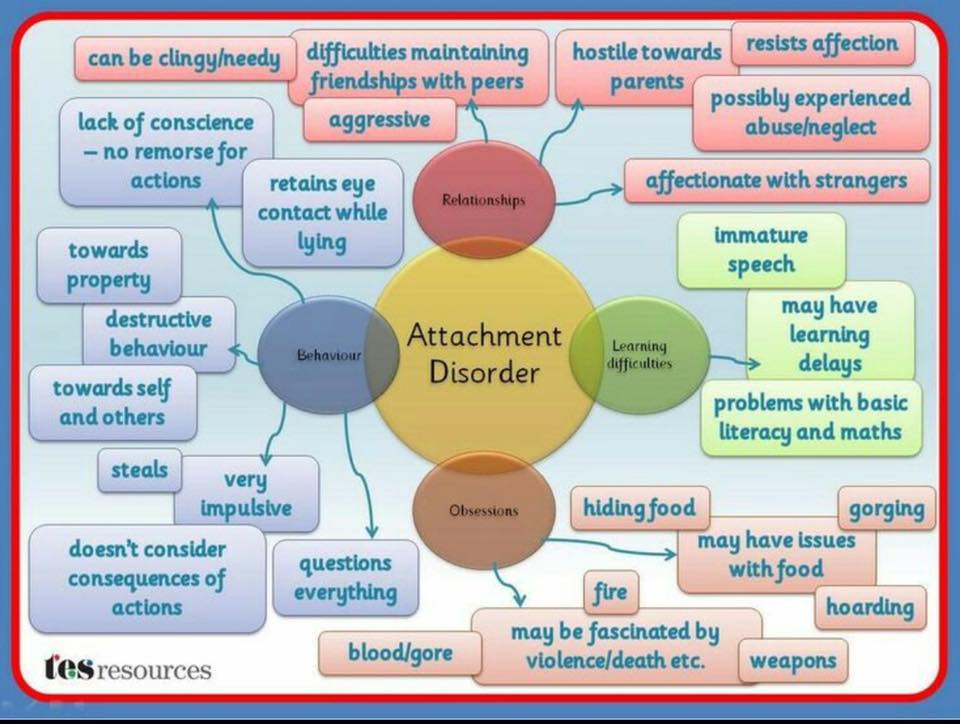
Signs and symptoms may include:
- Unexplained withdrawal, fear, sadness or irritability
- Sad and listless appearance
- Not seeking comfort or showing no response when comfort is given
- Failure to smile
- Watching others closely but not engaging in social interaction
- Failing to ask for support or assistance
- Failure to reach out when picked up
- No interest in playing peekaboo or other interactive games
When to see a doctor
Consider getting an evaluation if your child shows any of the signs above. Signs can occur in children who don’t have reactive attachment disorder or who have another disorder, such as autism spectrum disorder. It’s important to have your child evaluated by a pediatric psychiatrist or psychologist who can determine whether such behaviors indicate a more serious problem.
Causes
To feel safe and develop trust, infants and young children need a stable, caring environment. Their basic emotional and physical needs must be consistently met. For instance, when a baby cries, the need for a meal or a diaper change must be met with a shared emotional exchange that may include eye contact, smiling and caressing.
A child whose needs are ignored or met with a lack of emotional response from caregivers does not come to expect care or comfort or form a stable attachment to caregivers.
It’s not clear why some babies and children develop reactive attachment disorder and others don’t. Various theories about reactive attachment disorder and its causes exist, and more research is needed to develop a better understanding and improve diagnosis and treatment options.
Risk factors
The risk of developing reactive attachment disorder from serious social and emotional neglect or the lack of opportunity to develop stable attachments may increase in children who, for example:
- Live in a children’s home or other institution
- Frequently change foster homes or caregivers
- Have parents who have severe mental health problems, criminal behavior or substance abuse that impairs their parenting
- Have prolonged separation from parents or other caregivers due to hospitalization
However, most children who are severely neglected don’t develop reactive attachment disorder.
Complications
Without treatment, reactive attachment disorder can continue for several years and may have lifelong consequences.
Some research suggests that some children and teenagers with reactive attachment disorder may display callous, unemotional traits that can include behavior problems and cruelty toward people or animals. However, more research is needed to determine if problems in older children and adults are related to experiences of reactive attachment disorder in early childhood.
Prevention
While it’s not known with certainty if reactive attachment disorder can be prevented, there may be ways to reduce the risk of its development. Infants and young children need a stable, caring environment and their basic emotional and physical needs must be consistently met. The following parenting suggestions may help.
- Take classes or volunteer with children if you lack experience or skill with babies or children. This will help you learn how to interact in a nurturing manner.
- Be actively engaged with your child by lots of playing, talking to him or her, making eye contact, and smiling.
- Learn to interpret your baby’s cues, such as different types of cries, so that you can meet his or her needs quickly and effectively.
- Provide warm, nurturing interaction with your child, such as during feeding, bathing or changing diapers.
- Offer both verbal and nonverbal responses to the child’s feelings through touch, facial expressions and tone of voice.
Source
Diagnosis
A pediatric psychiatrist or psychologist can conduct a thorough, in-depth examination to diagnose reactive attachment disorder.
Your child’s evaluation may include:
- Direct observation of interaction with parents or caregivers
- Details about the pattern of behavior over time
- Examples of the behavior in a variety of situations
- Information about interactions with parents or caregivers and others
- Questions about the home and living situation since birth
- An evaluation of parenting and caregiving styles and abilities
Your child’s doctor will also want to rule out other psychiatric disorders and determine if any other mental health conditions co-exist, such as:
- Intellectual disability
- Other adjustment disorders
- Autism spectrum disorder
- Depressive disorders
Diagnostic and Statistical Manual of Mental Disorders (DMS-5)
Your doctor may use the diagnostic criteria for reactive attachment disorder in the DSM-5, published by the American Psychiatric Association. Diagnosis isn’t usually made before 9 months of age. Signs and symptoms appear before the age of 5 years.
Criteria include:
- A consistent pattern of emotionally withdrawn behavior toward caregivers, shown by rarely seeking or not responding to comfort when distressed
- Persistent social and emotional problems that include minimal responsiveness to others, no positive response to interactions, or unexplained irritability, sadness or fearfulness during interactions with caregivers
- Persistent lack of having emotional needs for comfort, stimulation and affection met by caregivers, or repeated changes of primary caregivers that limit opportunities to form stable attachments, or care in a setting that severely limits opportunities to form attachments (such as an institution)
- No diagnosis of autism spectrum disorder
Treatment
Children with reactive attachment disorder are believed to have the capacity to form attachments, but this ability has been hindered by their experiences.
Most children are naturally resilient. And even those who’ve been neglected, lived in a children’s home or other institution, or had multiple caregivers can develop healthy relationships. Early intervention appears to improve outcomes.
There’s no standard treatment for reactive attachment disorder, but it should involve both the child and parents or primary caregivers. Goals of treatment are to help ensure that the child:
- Has a safe and stable living situation
- Develops positive interactions and strengthens the attachment with parents and caregivers
Treatment strategies include:
- Encouraging the child’s development by being nurturing, responsive and caring
- Providing consistent caregivers to encourage a stable attachment for the child
- Providing a positive, stimulating and interactive environment for the child
- Addressing the child’s medical, safety and housing needs, as appropriate
Other services that may benefit the child and the family include:
- Individual and family psychological counseling
- Education of parents and caregivers about the condition
- Parenting skills classes
Controversial and coercive techniques
The American Academy of Child and Adolescent Psychiatry and the American Psychiatric Association have criticized dangerous and unproven treatment techniques for reactive attachment disorder.
These techniques include any type of physical restraint or force to break down what’s believed to be the child’s resistance to attachments — an unproven theory of the cause of reactive attachment disorder. There is no scientific evidence to support these controversial practices, which can be psychologically and physically damaging and have led to accidental deaths.
If you’re considering any kind of unconventional treatment, talk to your child’s psychiatrist or psychologist first to make sure it’s evidence based and not harmful.
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this disease.
Coping and support
If you’re a parent or caregiver whose child has reactive attachment disorder, it’s easy to become angry, frustrated and distressed. You may feel like your child doesn’t love you — or that it’s hard to like your child sometimes.
These actions may help:
- Educate yourself and your family about reactive attachment disorder. Ask your pediatrician about resources or check trusted internet sites. If your child has a background that includes institutions or foster care, consider checking with relevant social service agencies for educational materials and resources.
- Find someone who can give you a break from time to time. It can be exhausting caring for a child with reactive attachment disorder. You’ll begin to burn out if you don’t periodically have downtime. But avoid using multiple caregivers. Choose a caregiver who is nurturing and familiar with reactive attachment disorder or educate the caregiver about the disorder.
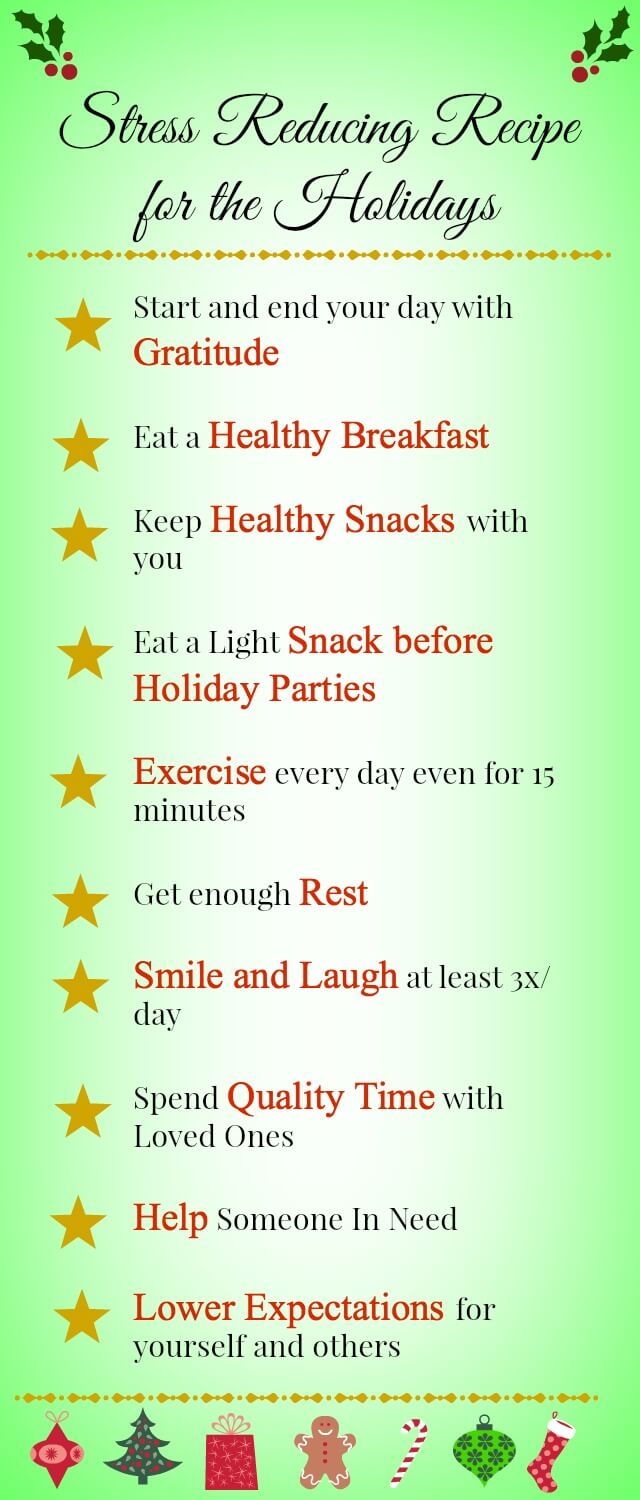
- Practice stress management skills. For example, learning and practicing yoga or meditation may help you relax and not get overwhelmed.
- Make time for yourself. Develop or maintain your hobbies, social engagements and exercise routine.
- Acknowledge it’s OK to feel frustrated or angry at times. The strong feelings you may have about your child are natural. But if needed, seek professional help.
Preparing for your appointment
You may start by visiting your child’s pediatrician. However, you may be referred to a child psychiatrist or psychologist who specializes in the diagnosis and treatment of reactive attachment disorder or a pediatrician specializing in child development.
Here’s some information to help you get ready and know what to expect from your doctor.
What you can do
Before your appointment, make a list of:
- Any behavior problems or emotional issues you’ve noticed, and include any signs or symptoms that may seem unrelated to the reason for your child’s appointment
- Key personal information, including any major stresses or life changes that you or your child have been through
- All medications, vitamins, herbal remedies or other supplements your child is taking, including the dosages
- Questions to ask your child’s doctor to make the most of your time together
Some basic questions to ask your doctor may include:
- What is likely causing my child’s behavior problems or emotional issues?
- Are there other possible causes?
- What kinds of tests does my child need?
- What’s the best treatment?
- What are the alternatives to the primary approach that you’re suggesting?
- My child has these other mental or physical health conditions. How can I best manage them together?
- Are there any restrictions that my child needs to follow?
- Should I take my child to see other specialists?
- Is there a generic alternative to the medicine you’re prescribing for my child?
- Are there any brochures or other printed material that I can have? What websites do you recommend?
- Are there social services or support groups available to parents in my situation?
What to expect from your doctor
Your child’s doctor or mental health provider is likely to ask you a number of questions. Be ready to answer them to reserve time to go over any points you want to spend more time on.
Some questions the doctor may ask include:
- When did you first notice problems with your child’s behavior or emotional responses?
- Have your child’s behavioral or emotional issues been continuous or occasional?
- How are your child’s behavioral or emotional issues interfering with his or her ability to function or interact with others?
- Can you describe your child’s and the family’s home and living situation since birth?
- Can you describe interactions with your child, both positive and negative?
Source